- Overview
- Log In For Videos
- Give Feedback
- Seizure Classification
- Unknown Onset Seizure
- Neonatal Seizure
- Epilepsy Classification
- Generalized Epilepsy
- Focal Epilepsy
- Generalized and Focal Epilepsy
- Unknown Epilepsy
- Epilepsy Syndromes
- Epilepsy Etiologies
- Metabolic Etiologies
- Immune Etiologies
- Infectious Etiologies
- Unknown Etiologies
- Encephalopathy
- Epilepsy imitators
SELF-LIMITED EPILEPSY WITH CENTROTEMPORAL SPIKES (SeLECTS)
Background
The background must be normal, with the presence of normal sleep architecture.
Interictal
High amplitude centrotemporal spike-, sharp- or sharp-waves that activate in drowsiness and sleep are mandatory. These may be unilateral or bilateral and are usually frequent. The centrotemporal spike/sharp has a typical triphasic morphology with a transverse dipole - maximum negativity in centrotemporal electrodes (C3/C4 and T3/T4) and maximum positivity frontally. Epileptiform abnormality may be seen in other areas (midline, parietal, frontal, occipital).
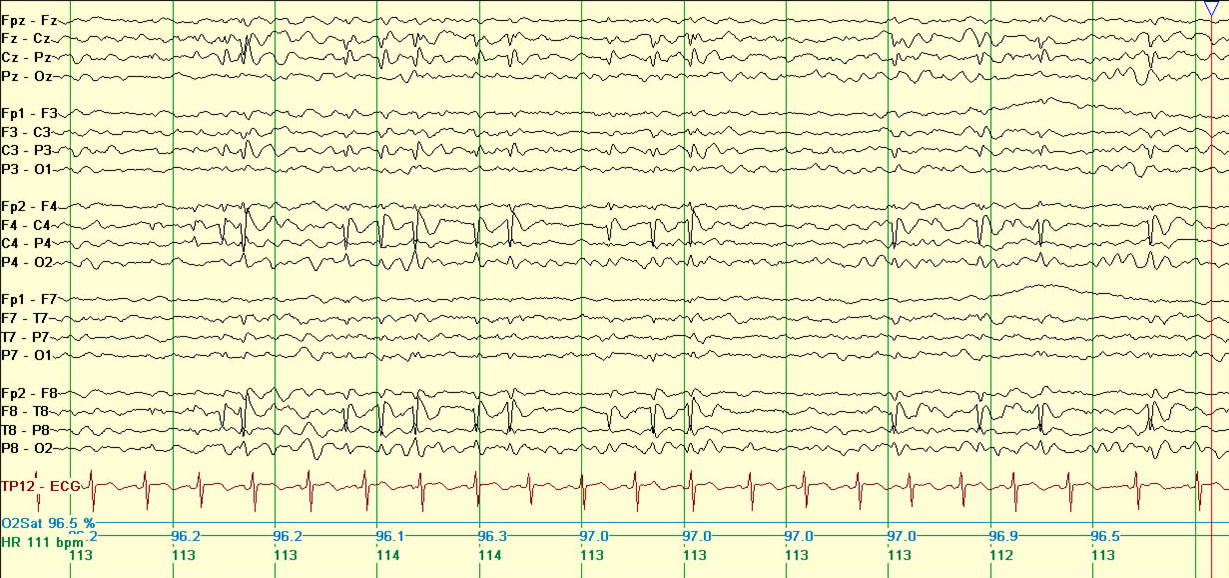
Example of centrotemporal sharp waves, bipolar montage.
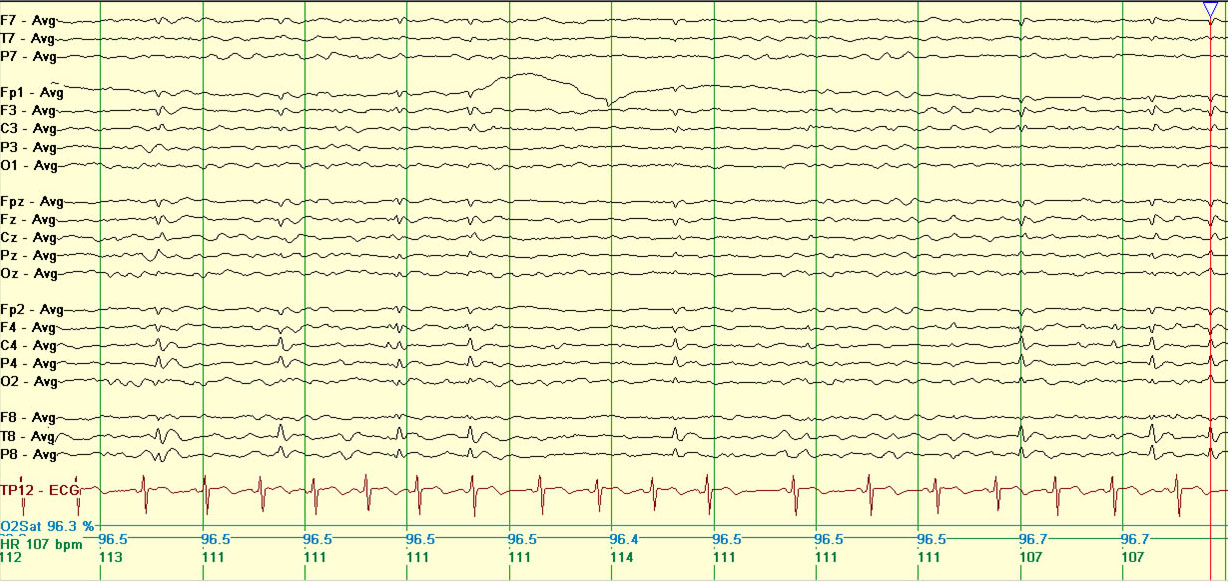
Example of centrotemporal sharp waves, referential montage.
CAUTION If marked activation in sleep  review for a history of language or cognitive regression (consider developmental and/or epileptic encephalopathy with spike-wave activation in sleep)
review for a history of language or cognitive regression (consider developmental and/or epileptic encephalopathy with spike-wave activation in sleep)
Activation
Epileptiform activity increases in drowsiness and sleep, when discharges often have a wider field and may become bilaterally synchronous. In 10-20% of children, centrotemporal discharges may be activated by sensory stimulation of the fingers or toes.

Example of EEG in the awake state.
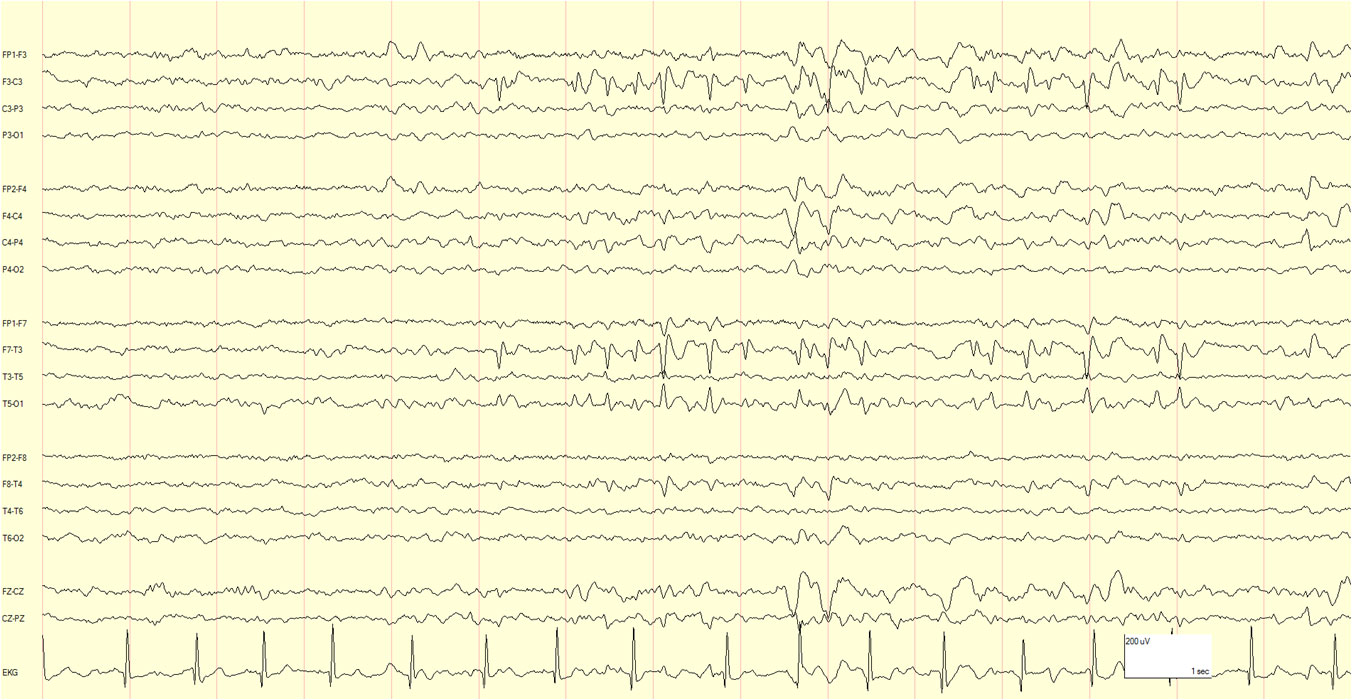
Example of EEG in the same patient, showing activation in sleep.
Ictal
Seizures are infrequent, so it is rare to obtain an ictal recording and there are few published reports of these in the literature. Seizures may be accompanied by a brief decrease in amplitude of the background EEG, followed by diffuse sharp-wave discharges of increasing amplitude, predominantly in one centrotemporal region. In a focal to bilateral tonic-clonic seizure, the ictal discharges become bilaterally synchronous (as opposed to generalized).
This website is owned by the International League Against Epilepsy. Text on this website, last updated June 30, 2024,
is available under a Creative Commons Attribution-ShareAlike 4.0 International License,
EXCEPTING all videos and images, which remain copyrighted by the International League Against Epilepsy.