- Overview
- Log In For Videos
- Give Feedback
- Seizure Classification
- Unknown Onset Seizure
- Neonatal Seizure
- Epilepsy Classification
- Generalized Epilepsy
- Focal Epilepsy
- Generalized and Focal Epilepsy
- Unknown Epilepsy
- Epilepsy Syndromes
- Epilepsy Etiologies
- Metabolic Etiologies
- Immune Etiologies
- Infectious Etiologies
- Unknown Etiologies
- Encephalopathy
- Epilepsy imitators
CHILDHOOD ABSENCE EPILEPSY (CAE)
Background
The background is normal. Occipital intermittent rhythmic delta activity (OIRDA) may be seen in around 20% of cases.
CAUTION Focal slowing seen consistently in one area  consider structural brain abnormality.
consider structural brain abnormality.
CAUTION Generalized slowing is not seen.
Interictal
2.5-4Hz generalized spike-wave, or fragments of generalized spike-wave are seen in the interictal EEG. These are brief (usually <2 second) and most commonly seen in sleep.
CAUTION Although focal
spikes (as fragments of generalized spike-wave) can occur, if
they consistently arise in one area
consider structural brain abnormality.
Activation
EEG abnormality and absence seizures are provoked by hyperventilation. If hyperventilation is poorly performed, generalized spike-wave may not be seen.
Intermittent photic stimulation provokes generalized spike-wave in 15-20% of individuals but does not provoke seizures.
EEG abnormality is enhanced by sleep deprivation, in drowsiness and in sleep. Generalized spike-wave often becomes fragmented with sleep deprivation or in sleep. Fragmented generalized spike-wave can appear focal or multi-focal but usually is not consistently seen in one area. The morphology of the focal spike-wave typically appears similar to the generalized spike-wave.
CAUTION Where hyperventilation is performed well for three minutes and no generalized spike-wave is seen in an untreated patient, childhood absence epilepsy is excluded.
Ictal
Regular 3Hz (range 2.5-4Hz) generalized spike-wave occurs associated with absence seizures. Polyspike-wave can occur in the ictal EEG.
CAUTION Slow spike-wave (<2.5Hz) is exclusionary.
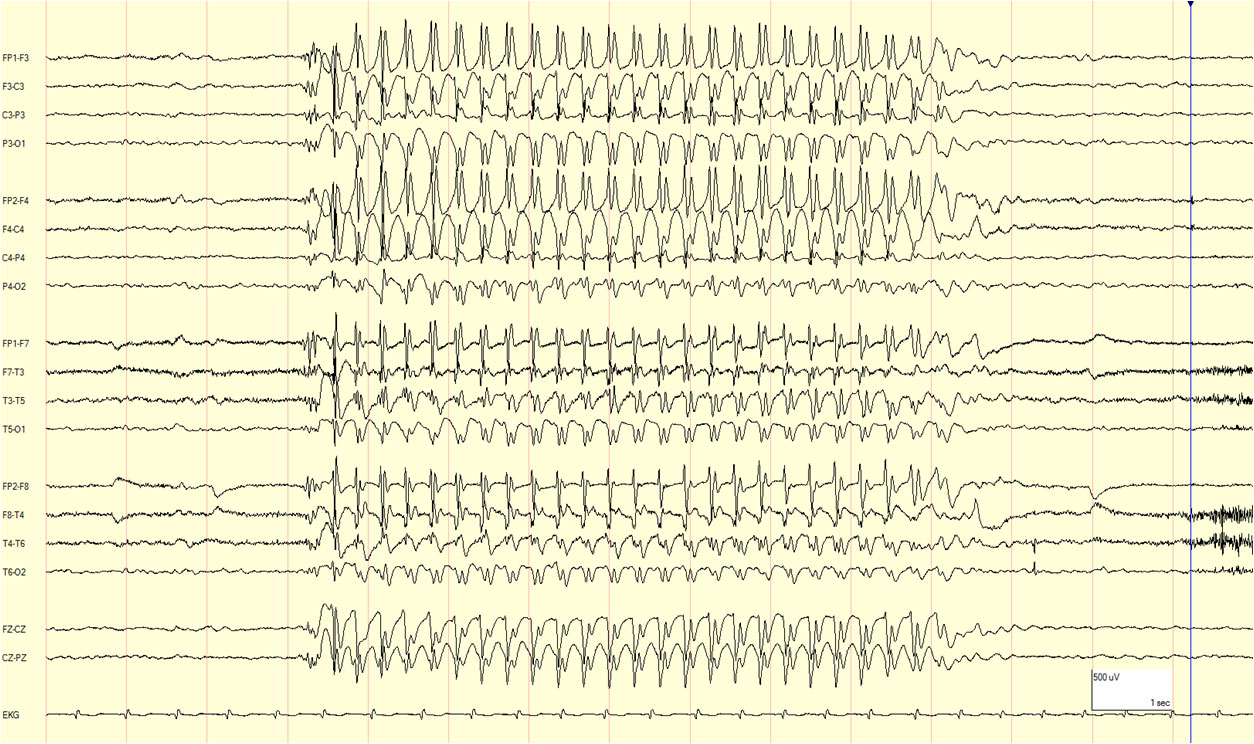
Example of 3Hz generalized spike-wave seen on the ictal EEG
This website is owned by the International League Against Epilepsy. Text on this website, last updated June 30, 2024,
is available under a Creative Commons Attribution-ShareAlike 4.0 International License,
EXCEPTING all videos and images, which remain copyrighted by the International League Against Epilepsy.